Overview
Leg length discrepancy (LLD) affects about 70% of the general population, and can be either structural - when the difference occurs in bone structures - or functional, because of mechanical changes at the lower limbs. The discrepancy can be also classified by its magnitude into mild, intermediate, or severe. Mild LLD has been particularly associated with stress fracture, low back pain and osteoarthritis, and when the discrepancy occurs in subjects whose mechanical loads are increased by their professional, daily or recreational activities, these orthopaedic changes may appear early and severely. The aim of this study was to analyze and compare ground reaction force (GRF) during gait in runners with and without mild LLD. Results showed that subjects with mild LLD of 0.5 to 2.0 cm presented higher values of minimum vertical GRF (0.57 ? 0.07 BW) at the shorter limb compared to the longer limb (0.56 ? 0.08 BW) Therefore, subjects with mild LLD adopt compensatory mechanisms that cause additional overloads to the musculoskeletal system in order to promote a symmetrical gait pattern as showed by the values of absolute symmetric index of vertical and horizontal GRF variables.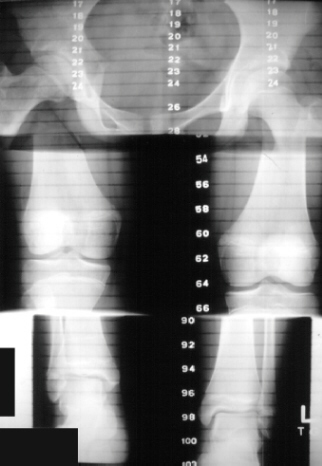
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding.
Diagnosis
A doctor will generally take a detailed medical history of both the patient and family, including asking about recent injuries or illnesses. He or she will carefully examine the patient, observing how he or she moves and stands. If necessary, an orthopedic surgeon will order X-ray, bone age determinations and computed tomography (CT) scans or magnetic resonance imaging (MRI).
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.

how to grow taller exercises
Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
Leg length discrepancy (LLD) affects about 70% of the general population, and can be either structural - when the difference occurs in bone structures - or functional, because of mechanical changes at the lower limbs. The discrepancy can be also classified by its magnitude into mild, intermediate, or severe. Mild LLD has been particularly associated with stress fracture, low back pain and osteoarthritis, and when the discrepancy occurs in subjects whose mechanical loads are increased by their professional, daily or recreational activities, these orthopaedic changes may appear early and severely. The aim of this study was to analyze and compare ground reaction force (GRF) during gait in runners with and without mild LLD. Results showed that subjects with mild LLD of 0.5 to 2.0 cm presented higher values of minimum vertical GRF (0.57 ? 0.07 BW) at the shorter limb compared to the longer limb (0.56 ? 0.08 BW) Therefore, subjects with mild LLD adopt compensatory mechanisms that cause additional overloads to the musculoskeletal system in order to promote a symmetrical gait pattern as showed by the values of absolute symmetric index of vertical and horizontal GRF variables.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding.
Diagnosis
A doctor will generally take a detailed medical history of both the patient and family, including asking about recent injuries or illnesses. He or she will carefully examine the patient, observing how he or she moves and stands. If necessary, an orthopedic surgeon will order X-ray, bone age determinations and computed tomography (CT) scans or magnetic resonance imaging (MRI).
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.
how to grow taller exercises
Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
